Open Scalpel-Bougie Cricothyroidotomy
Endotracheal intubation is first line for securing the airway. In a 'cannot intubate, cannot oxygenate' (CICO) situation, cricothyroidotomy can buy time (minutes) while expert help or definitive treatment is organised.
The aim is to insert the largest diameter tube in the least amount of time with the fewest complications.
The 4th National Audit Project 2011 (NAP4) of the Royal College of Anaesthetists reported that:
Needle cricothyroidotomy and Mini-Trach/Seldinger techniques are quick but have a higher failure rate
Once help arrives, the open technique takes only slightly longer and has a lower failure rate
More recently, the Royal College of Anaesthetists and ENT UK have developed a consensus statement available here. The recommendation is that the standard 'front of neck airway' or FONA should be a scalpel-bougie cricothyroidotomy.
Do not hesitate to call for expert help or equipment.
Below is a generic description of this procedure for reference purposes. You should seek specific advanced airway training (eg ALS, ATLS) rather than use this page as a manual.
BASIC EQUIPMENT
Disinfectant wipe/liquid
Personal protective equipment
Swabs
Scalpel and blade
Gum elastic bougie
Good light - preferably headlight
Tracheostomy dilator or artery forceps
Retractors eg small Langenbecks
Selection of tracheostomy tubes (eg size 4 to 8) and endotracheal tubes including paediatric sizes
Large suture (eg 0 or 1 gauge)
Ventilator, tubing, connectors - check with anaesthetist
Tube ties etc.
Plenty of assistance
You may have access to diathermy and other equipment
PROCEDURE
1. Aseptic technique insofar as possible given the situation. Quickly disinfect the skin.
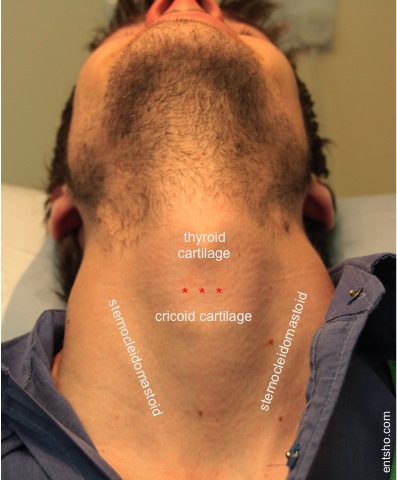
2. Hold the larynx firmly in your non-dominant hand to stabilise it.
3. Make a horizontal stab incision into the cricothyroid recess (red asterisks in the photo below). When making a stab incision, avoid cutting from side to side to minimise bleeding. The blade can be turned 90 degrees to help open the cricothyroidotomy. Alternatively make a vertical cut over the recess and dissect down through the cricothyroid membrane.
4. With retractors, a tracheostomy dilator, and/or a cricoid hook, dilate the hole.
5. Insert a gum elastic bougie, angled caudally into the airway.
6. Railroad a tracheostomy or endotracheal tube over the bougie under direct vision. Inflate the cuff. Someone must hold the tracheostomy tube in position. They must not let go until it has been secured. If unable to locate a tracheostomy tube or the smallest size does not fit, consider using a small oral endotracheal tube, taking care not to push the tube past the carina.

7. Check capnography, oximetry, chest signs etc. to confirm tube position.
8. Secure haemostasis.
9. Suture the tube flange (sutures can be removed when the situation is under control).
10. Pass tube ties through the tube flange.
11. Ventilate and reassess.
12. Perform a formal tracheostomy.
Link to ExR Virtual Reality: Cricothyroidotomy
Page last reviewed: 4 May 2024